
🦟 West Nile Virus (WNV) & Ocular Involvement
- Background:
- WNV is a mosquito-borne RNA flavivirus (mainly Culex and Aedes species).
- Most infections are asymptomatic (≈80%); ~20% cause flu-like illness; <1% cause neuroinvasive disease (meningoencephalitis).
- Ocular manifestations include anterior uveitis, vitritis, retinal vasculitis, optic neuritis, and most commonly chorioretinitis (>85% of ocular cases).
📄 Case 1
- Patient: 59-year-old man, severe right-eye vision loss after 15-day febrile illness.
- Findings:
- BCVA: 1/10 (right), 9/10 (left).
- Fundus: track-like cream lesions (left), foveal discoloration & optic disc pallor (right).
- Imaging: hyperautofluorescent lines, OCT changes, FA hyperfluorescence, OCTA flow void in right fovea.
- Diagnosis: Bilateral WNV chorioretinopathy confirmed by IgM & IgG serology; no CNS involvement on MRI.
- Treatment: Single intravitreal ranibizumab for macular edema.
- Outcome: Partial visual improvement; edema resolved but optic nerve pallor persisted.
- Significance: First reported ocular WNV case in Türkiye; highlights need for suspicion in endemic areas even without neurological symptoms.
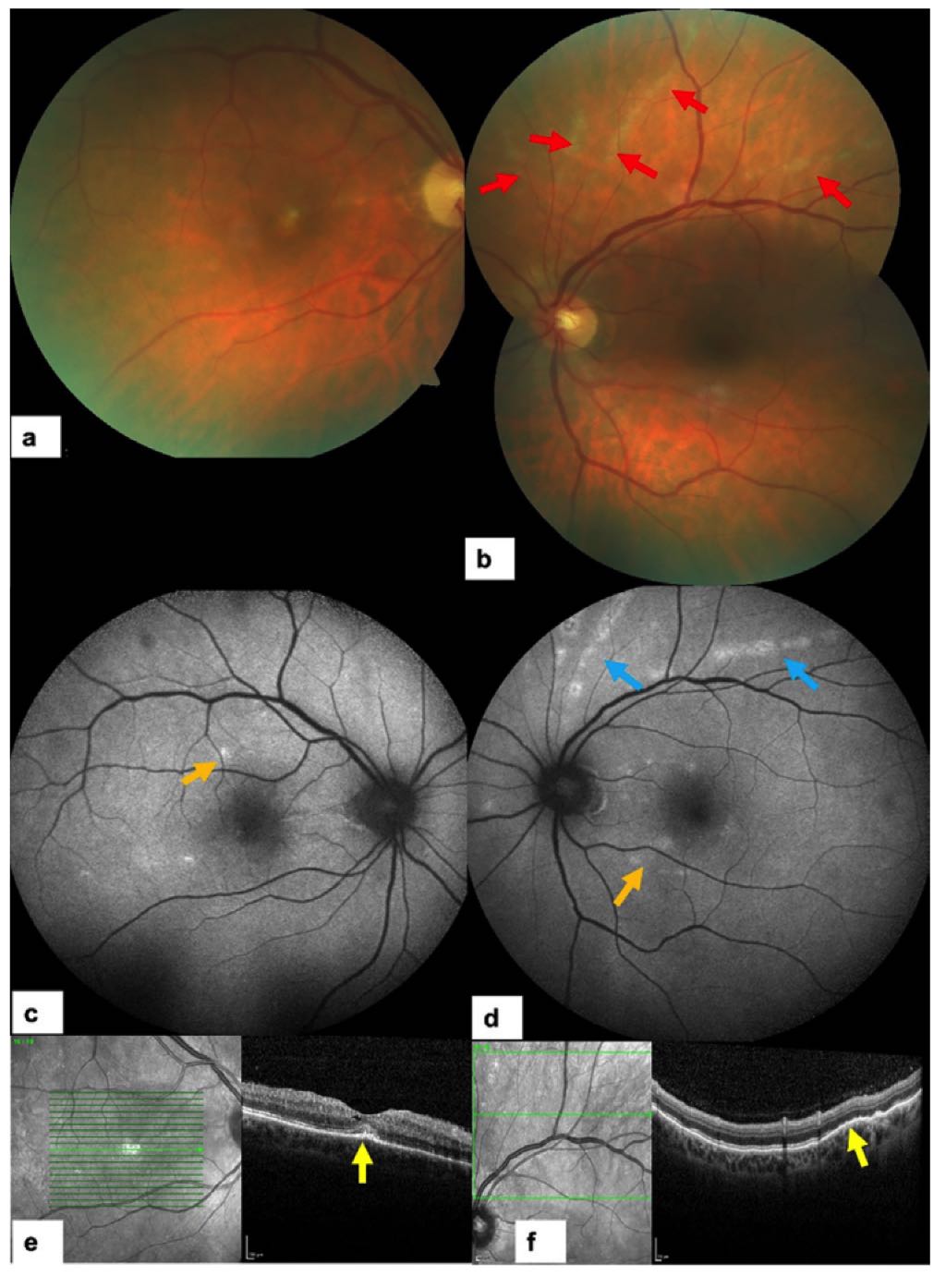
Figure 1 – First Presentation (August 2024)
-
(a) Right eye color fundus photo: Small whitish lesion at the foveal center.
-
(b) Left eye color fundus photo: Normal-appearing macula but with track-like cream-colored linear lesions in the superior retina (marked by red arrows).
-
(c) Right eye fundus autofluorescence (FAF): A few hyperautofluorescent macular spots (orange arrow).
-
(d) Left eye FAF: Linear hyperautofluorescent lesions extending from the posterior pole toward the periphery (blue arrows) plus a few hyperautofluorescent macular spots (orange arrow).
-
(e) Right eye OCT: Shows intraretinal cysts, subfoveal hyperreflective material (yellow arrow), hyperreflective dots in posterior vitreous, and focal RPE/EZ alterations.
-
(f) Left eye OCT over linear lesions: Focal RPE and EZ disruption with focal choroidal thickening (yellow arrow).
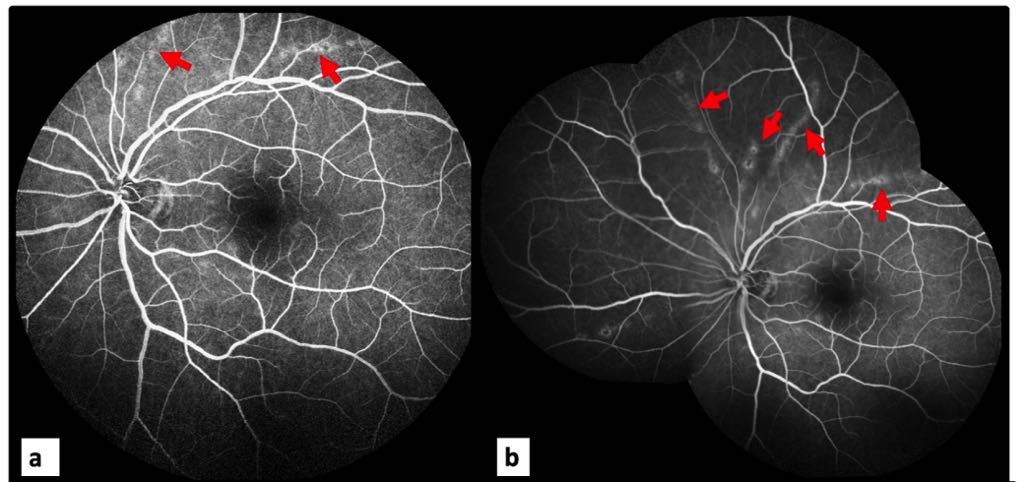
(a) & (b) FA: Linear hyperfluorescent lesions (red arrows) extending from posterior pole toward the periphery.
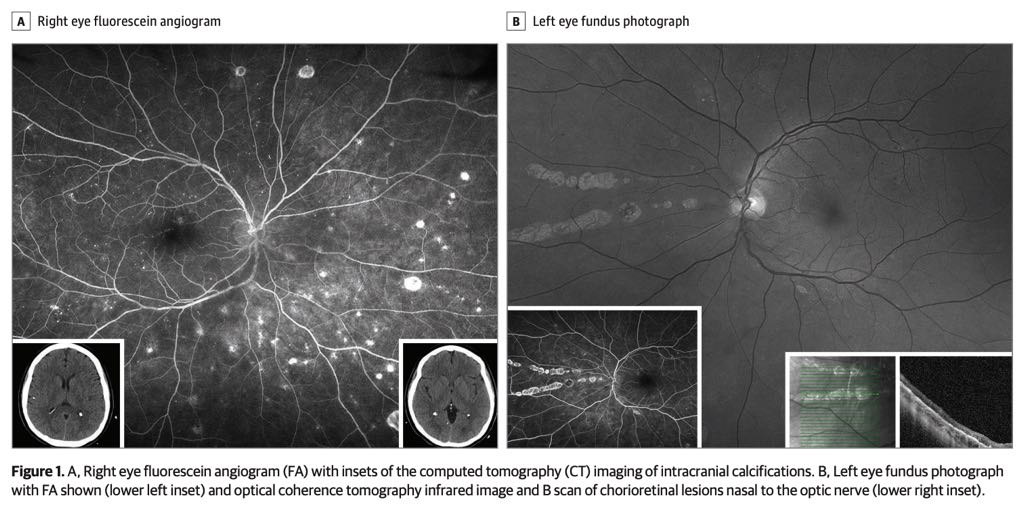
📄 Case 2
- Patient: 56-year-old woman with type 2 diabetes, recent febrile illness, and floaters in right eye after hospitalization for suspected sepsis.
- Findings:
- Moderate diabetic retinopathy, scattered & linear chorioretinal lesions, mild vitritis.
- OCT: retinal atrophy, RPE hypertrophy, choroidal hyperreflectivity.
- Diagnosis: WNV chorioretinitis confirmed by positive IgM & IgG; other infectious and autoimmune causes ruled out.
- Risk Factors: Age >45, diabetes, recent febrile illness.
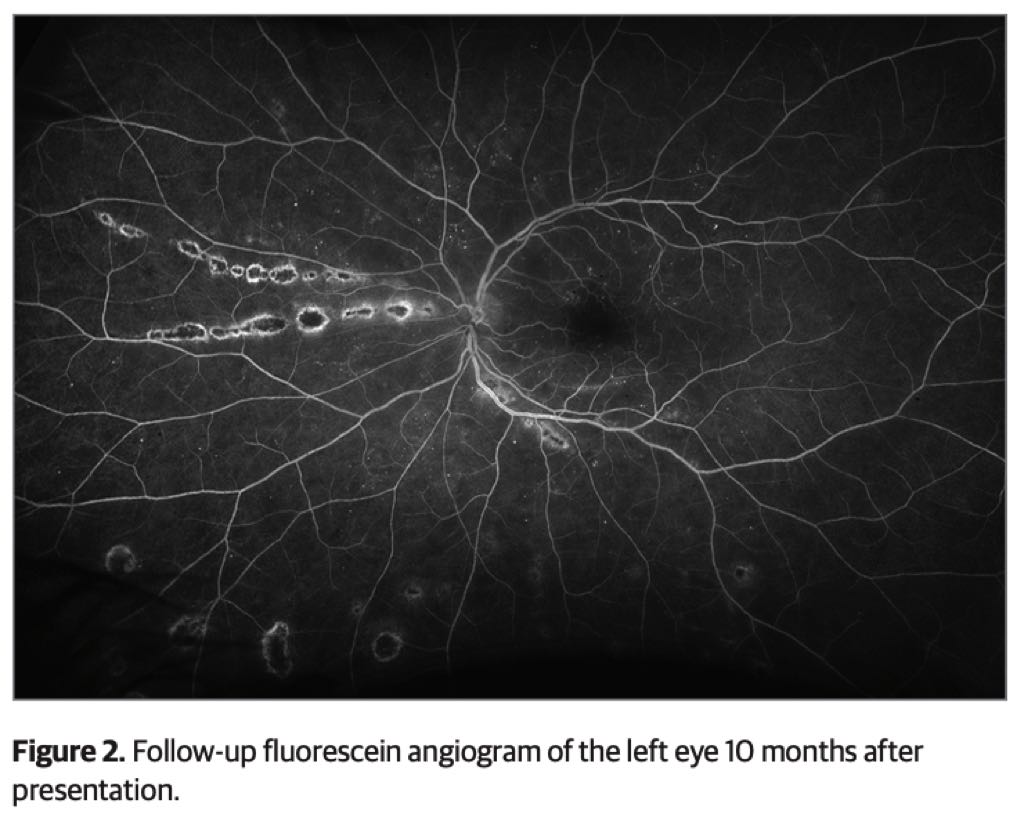
- Outcome: Symptoms and vitritis resolved with observation; lesions persisted.
🔍 Key Clinical Insights
- Diagnosis: Based on characteristic fundus lesions, multimodal imaging (FA, OCT, OCTA, autofluorescence), and WNV-specific IgM detection.
- Imaging Patterns: Linear/curvilinear lesions along retinal nerve fiber layer; target-like FA lesions; deep chorioretinal changes on OCT.
- Pathophysiology: Virus may spread hematogenously via choroid or neurally via optic nerve.
- Treatment: Mostly supportive; anti-VEGF (e.g., ranibizumab) for macular edema or CNV; steroids sometimes used but efficacy unclear.
- Prognosis: Often self-limiting; visual recovery may be partial if optic nerve damage occurs.
Here’s a side-by-side comparison of the two West Nile Virus (WNV) ocular cases from your document:
| Feature | Case 1 | Case 2 |
|---|---|---|
| Patient | 59-year-old man | 56-year-old woman |
| Medical History | Recent 15-day febrile illness; no CNS symptoms | Type 2 diabetes; recent febrile illness with syncope, headache, myalgias; hospitalized for suspected sepsis |
| Ocular Symptoms | Severe right-eye vision loss for 2 days | Floaters in right eye; vision otherwise normal |
| Visual Acuity (BCVA) | R: 1/10 → 2/10 after treatment; L: 9/10 → 10/10 | Normal |
| Fundus Findings | R: foveal discoloration, optic disc pallor; L: track-like cream lesions | Scattered & linear chorioretinal lesions; moderate diabetic retinopathy |
| Imaging |
FAF: hyperautofluorescent lines (L) & patches (OU) OCT: intraretinal cysts (R), RPE/EZ changes (OU) FA: hyperfluorescent lesions (OU) OCTA: flow void in R fovea |
FA: mild venular staining, no major leakage OCT: retinal atrophy, RPE hypertrophy, choroidal hyperreflectivity |
| Lab Findings | WNV IgM & IgG positive; PCR negative | WNV IgM & IgG positive; rheumatoid factor negative |
| Neurological Involvement | None (MRI normal) | Recent encephalitis suspected; CNS imaging without active lesions |
| Treatment | Single intravitreal ranibizumab (R eye) for macular edema | Observation only |
| Outcome | Macular edema resolved; partial vision improvement; persistent optic nerve pallor (R) | Symptoms & vitritis resolved; chorioretinal lesions persisted |
| Significance | First documented ocular WNV case in Türkiye; occurred without neurological symptoms | Highlights risk factors (age >45, diabetes) and classic lesion patterns even without severe vision loss |
Özkan Ö, Akdeniz A, Ayhan Z, Nazlı A, Saatci AO. West Nile Virus Chorioretinitis: First Case with Ocular Involvement in Türkiye. Turk J Ophthalmol. 2025;55(2):99‑104. doi:[10.4274/tjo.galenos.2025.05673]
Firn K, Youn J, Sierpina D. Fever and Floaters in a 56-Year-Old Woman. JAMA Ophthalmol. Published online January 16, 2025. doi:[10.1001/jamaophthalmol.2024.5862]