
Introduction
- Hypertension is the leading risk factor for cardiovascular disease (CVD) and mortality worldwide, projected to affect 1.56 billion people by 2025.
- Hypertension affects retinal, choroidal, and optic nerve circulations, leading to hypertensive retinopathy, choroidopathy, and optic neuropathy.
- Hypertension is a major risk factor for diabetic retinopathy, retinal artery/vein occlusion, retinal arterial macroaneurysm, and possibly age-related macular degeneration and glaucoma.
Hypertensive Retinopathy
- Definition and Classification:
- Hypertensive retinopathy results from acute and/or chronic elevated blood pressure, causing vasospasm, sclerotic changes, and blood-retinal barrier disruption.
- Stages (Mitchell-Wong grading system, 2004, high reliability):
- None: No detectable signs.
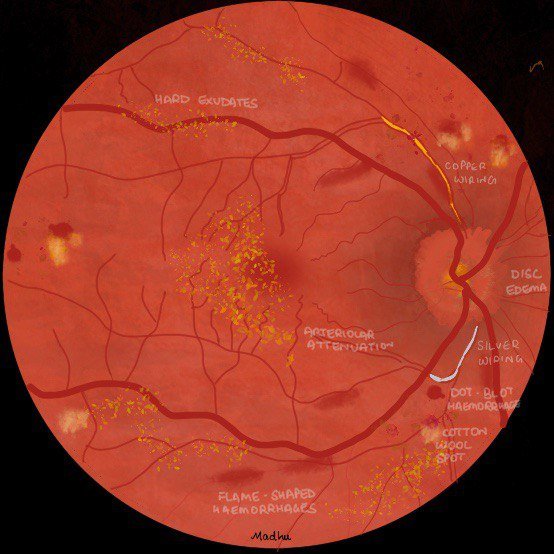
- Mild: Generalized/focal arteriolar narrowing, arteriovenous (AV) nicking, silver/copper wiring.
- Moderate: Retinal hemorrhages (blot, dot, flame-shaped), microaneurysms, cotton-wool spots, hard exudates.
- Malignant: Moderate retinopathy signs + optic disc swelling, often with severely elevated blood pressure.
- Phases (not always sequential): Vasoconstrictive (arteriolar narrowing), sclerotic (intimal thickening, AV nicking), exudative (hemorrhages, exudates), malignant (optic disc swelling).
- Pathophysiology includes inflammation, endothelial dysfunction, abnormal angiogenesis, and oxidative stress.
- Signs may occur in normotensive individuals, suggesting other mechanisms.
- Epidemiology:
- Prevalence of hypertensive retinopathy signs (except optic disc swelling) in adults ≥40 years: 2–17%, increasing with age.
- Higher prevalence in Chinese populations compared to Caucasians; men may have higher rates than women.
- Generalized arteriolar narrowing is an early preclinical marker of hypertension, predictive of incident hypertension (meta-analysis of 10,229 participants).
- Retinal arteriolar narrowing observed in children as young as 4–5 years, indicating early microvascular effects.
- Retinal venular widening may also be associated with hypertension, suggesting dynamic venular response.
- Systemic Associations:
- Stroke and Cerebrovascular Diseases:
- Moderate hypertensive retinopathy signs are strongly linked to subclinical (MRI-defined) cerebral infarction, white matter lesions, atrophy, and microbleeds.
- Associated with incident clinical stroke and lacunar stroke, even after controlling for risk factors.
- Retinal arteriolar narrowing linked to lacunar stroke; hemorrhages linked to cerebral hemorrhages.
- Retinal venular widening associated with hemorrhagic stroke.
- Hypertensive retinopathy is associated with cognitive decline and dementia; retinal vascular density changes linked to Alzheimer’s disease.
- Heart Disease:
- Associated with coronary artery calcification, aortic stiffness, left ventricular hypertrophy, and carotid intima-media thickness.
- Moderate hypertensive retinopathy increases risk of congestive heart failure (3x) and coronary artery disease events.
- Higher prevalence in heart failure with preserved ejection fraction.
- Kidney Disease:
- Cross-sectional association with chronic kidney disease (CKD) and renal impairment.
- Coexistence of retinopathy with microalbuminuria and left ventricular hypertrophy increases CVD and CKD progression risk.
- Mortality:
- Moderate hypertensive retinopathy is associated with increased CVD, stroke, and coronary heart disease mortality, comparable to diabetes risk.
- Mild retinopathy signs also linked to CVD mortality in hypertensive patients.
- Stroke and Cerebrovascular Diseases:
Hypertensive Choroidopathy
- Less common than retinopathy, caused by choroidal ischemia leading to retinal pigment epithelium (RPE) and retinal disruption.
- Signs: Elschnig spots (gray-yellow RPE lesions), Siegrist streaks (hyperpigmented streaks along choroidal arteries), choroidal thickening (via OCT), and serous retinal detachment in severe cases.
- Can lead to vision loss.
Hypertensive Optic Neuropathy
- Bilateral optic disc swelling is a hallmark of malignant hypertensive retinopathy, strongly correlated with CVD risk and mortality.
- Pathogenesis controversial: ischemia, raised intracranial pressure (papilledema), or hypertensive encephalopathy.
- Requires urgent antihypertensive management.
Emerging Imaging Technologies
- Assessment of Retinal Vascular Branching and Geometry:
- Digital fundus photography and software (e.g., SIVA, VAMPIRE, QUARTZ) quantify retinal vascular caliber, tortuosity, fractal dimension, and branching angles.
- Deviations from optimal vascular geometry indicate impaired microcirculatory efficiency and increased vascular damage risk.
- Optical Coherence Tomography Angiography (OCTA):
- Non-invasive visualization of retinal capillary networks, detecting early microvascular changes in hypertension.
- Correlates with hypertensive retinopathy scores and systemic vascular risk factors.
- Paracentral acute middle maculopathy (PAMM) may be an early retinal microvascular change in hypertension.
- Telemedicine and Smartphone:
- Telescreening with fundus photography is cost-effective for detecting hypertensive retinopathy.
- Smartphone fundus photography is reliable, portable, and useful in acute hypertension settings (e.g., emergency departments).
- Artificial Intelligence (AI):
- Deep learning with convolutional neural networks (CNNs) enables automated detection of hypertensive retinopathy, choroidopathy, and optic neuropathy, rivaling specialist accuracy.
- AI predicts CVD risk factors (e.g., blood pressure, BMI) from retinal photographs with high accuracy.
- Potential to improve decision-making and screening efficiency.
Future Directions
- Exploration of other ocular technologies: structural OCT, swept-source OCT, adaptive optics, retinal oximetry, and dynamic vessel analysis.
- Genetic studies identify loci associated with retinal vascular caliber and hypertensive retinopathy, aiding understanding of microcirculatory mechanisms.
- Regression of retinopathy signs with antihypertensive treatment (e.g., ACE inhibitors) is associated with better outcomes for left ventricular hypertrophy and target organ damage.
Conclusions
- Hypertensive retinopathy signs are common in adults and are markers of systemic vascular disease, predicting preclinical changes in cerebral, coronary, and renal microcirculations.
- Presence of hypertensive retinopathy indicates need for aggressive blood pressure management and CVD risk assessment, as per major guidelines (JNC, ESC/ESH, ACC/AHA, NICE).

Malignant Hypertension and PRES
-
Clinical Presentation of Malignant Hypertension:
-
Severe bilateral optic disc edema, retinal hemorrhages, cotton-wool spots, and macular exudates are hallmark findings.
-
Gradual vision decrease over weeks, often with best-corrected visual acuity reduced (e.g., 20/100 OD, 20/70 OS).
-
Systemic symptoms may include worsening headaches, numbness, and tinnitus, but no transient visual obscurations.
-
Malignant hypertension is defined by substantially elevated blood pressure with ischemic end-organ damage (retina, kidney, heart, brain).
-
-
Funduscopic Findings:
-
Earliest sign: Arteriolar narrowing due to vasospasm and increased vascular tone.
-
Chronic hypertension leads to arteriovenous nicking and “copper wiring” from intimal thickening and media hyperplasia.
-
Advanced findings include microaneurysms, hemorrhages, hard exudates, and cotton-wool spots due to blood-retina barrier disruption and necrosis.
-
Papilledema is a hallmark of malignant hypertension, distinguishing it from chronic hypertension.
-
Choroidopathy may present with Siegrist streaks (pigmented streaks along choroidal arteries) and Elschnig spots (gray-yellow or hyperpigmented choroidal lesions).
-
-
Posterior Reversible Encephalopathy Syndrome (PRES):
-
PRES is characterized by reversible subcortical vasogenic edema, most commonly caused by hypertension.
-
MRI shows diffuse T2-weighted signal abnormalities on fluid-attenuated inversion recovery sequences involving cerebral hemispheres, brainstem, and cerebellum.
-
Symptoms include headache, seizures, encephalopathy, and decreased vision.
-
PRES is diagnosed by clinical and radiographic evidence, with resolution typically following hypertension treatment.
-
-
Diagnostic Approach:
-
First step: Measure blood pressure to confirm malignant hypertension (e.g., 263/164 mm Hg in this case).
-
Lumbar puncture, corticosteroids, or antibiotics (e.g., azithromycin) are not indicated until hypertension is ruled out.
-
Differential diagnosis includes CNS/retinal vasculitis, inflammatory diseases (SLE, sarcoidosis), infectious encephalitis, neoplasms, and paraneoplastic encephalitis.
-
-
Complications of Malignant Hypertension:
-
Predisposes to arterial/venous occlusion, macroaneurysm, and ischemic optic neuropathy.
-
Persistent visual field defects and optic nerve pallor may occur due to ischemic optic neuropathy.
-
Choroidal ischemia may lead to visible Elschnig spots post-treatment.
-
-
Treatment and Outcome:
-
Immediate admission for intravenous antihypertensive medications.
-
Treatment of hypertension leads to marked improvement in retinopathy, optic neuropathy, and resolution of vasogenic edema on MRI.
-
Visual acuity may improve significantly (e.g., to 20/40 OD, 20/25 OS), but some visual field defects may persist.
-
-
Citation:
-
Xu SC, Chen JJ. Abnormal Magnetic Resonance Imaging Findings in a Patient With Optic Disc Edema, Retinal Hemorrhage, and Decreased Vision. JAMA Ophthalmology. 2018;136(1):92-93. doi:10.1001/jamaophthalmol.2017.4047
-