-
Definition: Superior Segmental Optic Nerve Hypoplasia (SSONH), also known as “topless optic disc,” is a congenital condition characterized by reduced regional ganglion cells (RGCs) in the superior optic disc.
-
Characteristic Findings (4 key features):
-
Superior entrance of the central retinal artery.
-
Superior optic disc pallor.
-
Thinning of the superior retinal nerve fiber layer (RNFL).
-
Inferior altitudinal or sectoral visual field (VF) defects.
-
-
Epidemiology: Rare condition, often underdiagnosed; commonly associated with maternal diabetes.
-
Etiology/Pathophysiology:
-
Pathogenesis is unclear but linked to maternal diabetes, suggesting a developmental insult to the superior optic nerve during embryogenesis.
-
Involves overproduction and subsequent elimination of retinal axons, as seen in human fetal optic nerve development.
-
-
Risk Factors:
-
Maternal diabetes mellitus (strong association, especially gestational diabetes).
-
High glucose levels may affect retinal patterning during embryogenesis, leading to neuronal death or altered retinal Müller cell function.
-
-
Clinical Presentation:
-
Patients typically have normal visual acuity but present with inferior visual field defects (altitudinal or sectoral).
-
Often asymptomatic unless visual field loss is significant, detected during routine screening.
-
-
Diagnostic Tools:
-
Fundus Examination: Shows superior disc pallor and superior entrance of the central retinal artery.
-
Optical Coherence Tomography (OCT): Reveals thinning of the superior RNFL and confirms optic disc hypoplasia.
-
OCT Angiography: Demonstrates reduced radial peripapillary capillary density in the superior segment.
-
Visual Field Testing: Confirms inferior altitudinal or sectoral defects, a critical diagnostic clue.
-
-
Differential Diagnosis:
-
Glaucoma: SSONH can mimic glaucomatous optic neuropathy due to RNFL thinning and VF defects but lacks progressive rim loss or elevated intraocular pressure.
-
Other optic nerve hypoplasias, optic atrophy, or congenital disc anomalies.
-
-
Management:
-
No specific treatment; management focuses on monitoring for associated conditions (e.g., diabetes-related complications).
-
Regular follow-up with OCT and VF testing to assess stability, as SSONH is non-progressive.
-
-
Prognosis:
-
Stable condition with no progression over time, unlike glaucoma.
-
Visual field defects are permanent but typically do not worsen.
-
-
Historical Context: First described by Petersen and Walton in 1977 in children born to diabetic mothers; termed SSONH by Robert K. in 1989.
Citation
Vickers, A., Zhou, A., Al-Zubidi, N., & Tripathy, K. (2024). Superior Segmental Optic Nerve Hypoplasia (SSONH). EyeWiki, American Academy of Ophthalmology. Last edited December 3, 2024. Retrieved from https://eyewiki.aao.org/Superior_Segmental_Optic_Nerve_Hypoplasia

-
Patient Presentation: A 15-year-old boy with high myopia (-11.00 diopters), axial length of 27.14 mm, and anisometropic amblyopia in the right eye, presenting with best-corrected visual acuity of 20/200.
-
Ocular Findings:
-
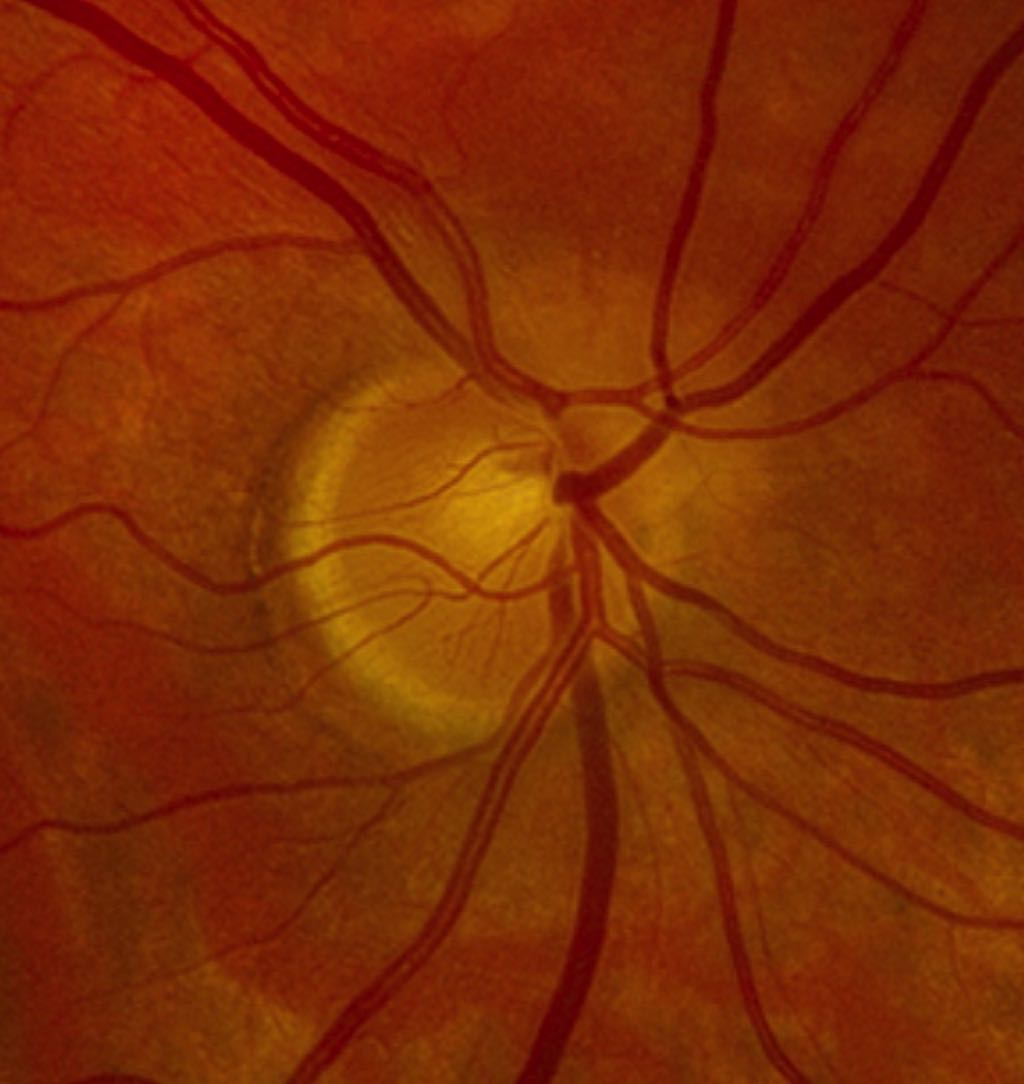
Segmental temporal optic nerve hypoplasia, characterized by a crescent-shaped disc with temporal hypoplasia.
-
Nearly absent optic cup, an exceptionally rare finding.
-
Left eye was unremarkable, indicating unilateral involvement.
-
-
Diagnostic Imaging:
-
Color fundus photograph and red-free image: Show a crescent-shaped disc with temporal hypoplasia (red arrowhead).
-
Optical Coherence Tomography (OCT): Confirms segmental temporal hypoplasia of the optic disc with a nearly absent cup.
-
-
Clinical Context: Segmental optic nerve hypoplasia is a rare variant of optic nerve hypoplasia, distinct from diffuse hypoplasia or aplasia.
-
Associated Conditions:
-
High myopia and elongated axial length (27.14 mm) may contribute to optic disc anomalies.
-
Anisometropic amblyopia likely explains poor visual acuity in the affected eye.
-
-
Rarity: Segmental temporal hypoplasia with an almost absent cup is exceptionally rare, making it a critical point for differentiation from other optic nerve anomalies.
-
Differential Diagnosis:
-
Optic nerve aplasia, diffuse optic nerve hypoplasia, or myopic disc changes.
-
Consider other congenital optic disc anomalies (e.g., morning glory disc anomaly, optic pit).
-
-
Management Implication: No specific treatment for segmental hypoplasia; focus on managing amblyopia and monitoring for myopic complications (e.g., retinal detachment, myopic maculopathy).
Citation
Palaniva, S., & Rajendran, A. (2024). Segmental Optic Nerve Hypoplasia. Ophthalmology Retina, e31. https://doi.org/10.1016/j.oret.2024.08.002