Superiority Trial: A type of randomized controlled trial designed to show that one treatment is better than another (or placebo/standard care).
Equivalence Trial: A type of randomized controlled trial designed to show that two treatments are essentially the same in effect.
Noninferiority Trial: A type of randomized controlled trial designed to show that a new treatment is no worse than an established standard treatment, often because the new treatment offers other advantages like lower cost or improved safety.
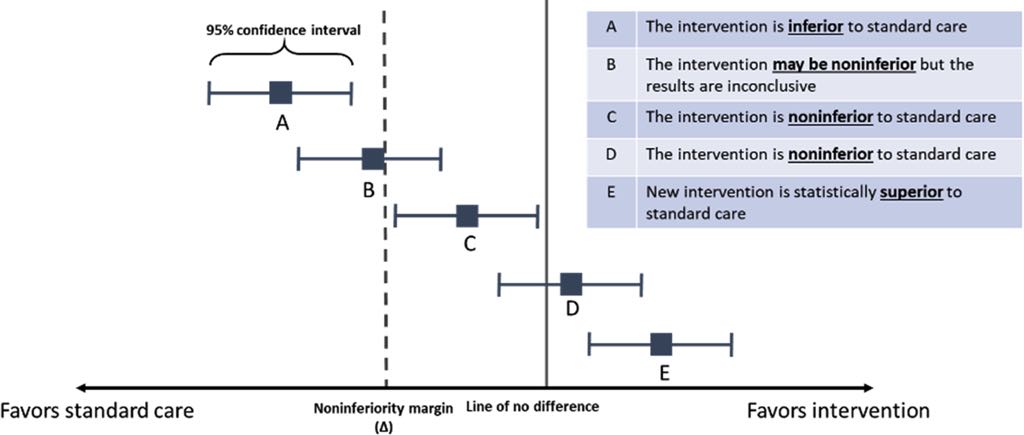
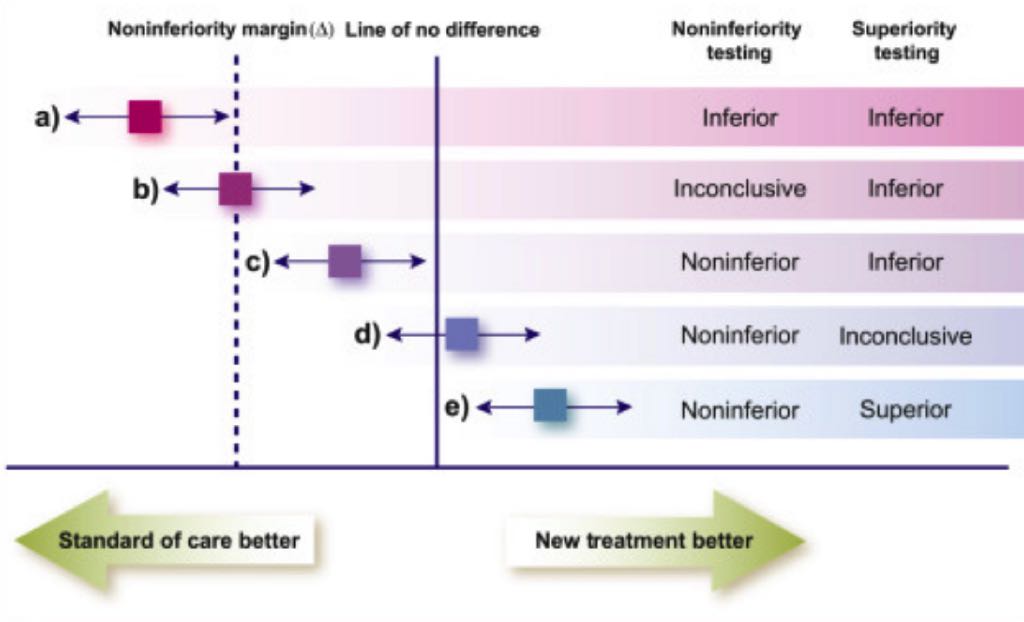
Noninferiority Margin: A pre-specified maximum acceptable difference in effect size between the new treatment and the standard treatment, below which the new treatment is considered noninferior.
Confidence Interval (CI): A range of values that is likely to contain the true effect size difference between two treatments, based on the trial data.
Line of No Difference: In a graphical representation of trial results, the point or line indicating zero difference in effect between the two treatments being compared.
Intention-to-Treat (ITT) Analysis: An analysis strategy where all patients are analyzed in the group to which they were originally randomized, regardless of whether they received or completed the assigned treatment.
Per-Protocol (PP) Analysis: An analysis strategy that includes only those patients who completed the trial according to the predefined protocol without major deviations.
Biocreep: The potential for a gradual degradation of treatment effects over time if slightly inferior interventions are consistently declared acceptable through noninferiority trials, setting a lower bar for subsequent interventions.
Allocation Concealment: A procedure that prevents researchers from knowing which treatment assignment a patient will receive before the patient is enrolled in the trial, helping to prevent selection bias.
Tips:
The primary goal of a noninferiority trial is to demonstrate that a new treatment is no worse than an existing standard treatment, whereas a superiority trial aims to prove that one treatment is better than another.
Researchers might choose a noninferiority trial when a new intervention is cheaper or safer than the old standard, making it preferable even if its effectiveness is only equivalent or slightly less.
The noninferiority margin is a predetermined effect size difference deemed small enough not to matter clinically. Defining it is crucial because it affects both the required sample size and the interpretation of the trial results.
One criterion is that the confidence interval of the difference in effect must exclude a predetermined effect size deemed small enough not to matter (the noninferiority margin), indicating that the new treatment’s inferiority is within the acceptable limit. (Alternatively, the confidence interval can include 0, suggesting any difference is due to chance, and exclude the noninferiority margin).
One criticism is that noninferiority trials can reward sloppiness, meaning imperfections in trial design (like an insensitive assay or a wide margin) can make it easier to falsely declare noninferiority.
A wide noninferiority margin makes it easier for the confidence interval of the treatment difference to fall within the acceptable range, potentially declaring noninferiority even if a clinically meaningful difference exists.
Biocreep is the concern that if slightly inferior interventions are repeatedly accepted as noninferior, the standard of care could gradually worsen over time as each new intervention only needs to clear a lower bar set by the previous acceptable intervention.
In superiority trials, ITT analysis is typically more conservative, while in noninferiority trials, ITT analysis can sometimes make it easier to demonstrate noninferiority by potentially diminishing the observed difference between groups.
Suboptimal administration of the standard care (e.g., subtherapeutic dose) can be a trial design deficiency that makes the new intervention and standard care appear more similar than they truly are, facilitating a noninferiority declaration.
Clinicians should use their expertise to assess the chosen noninferiority margin and consider whether patients would perceive the magnitude of the potential loss of treatment efficacy represented by that margin as clinically important.