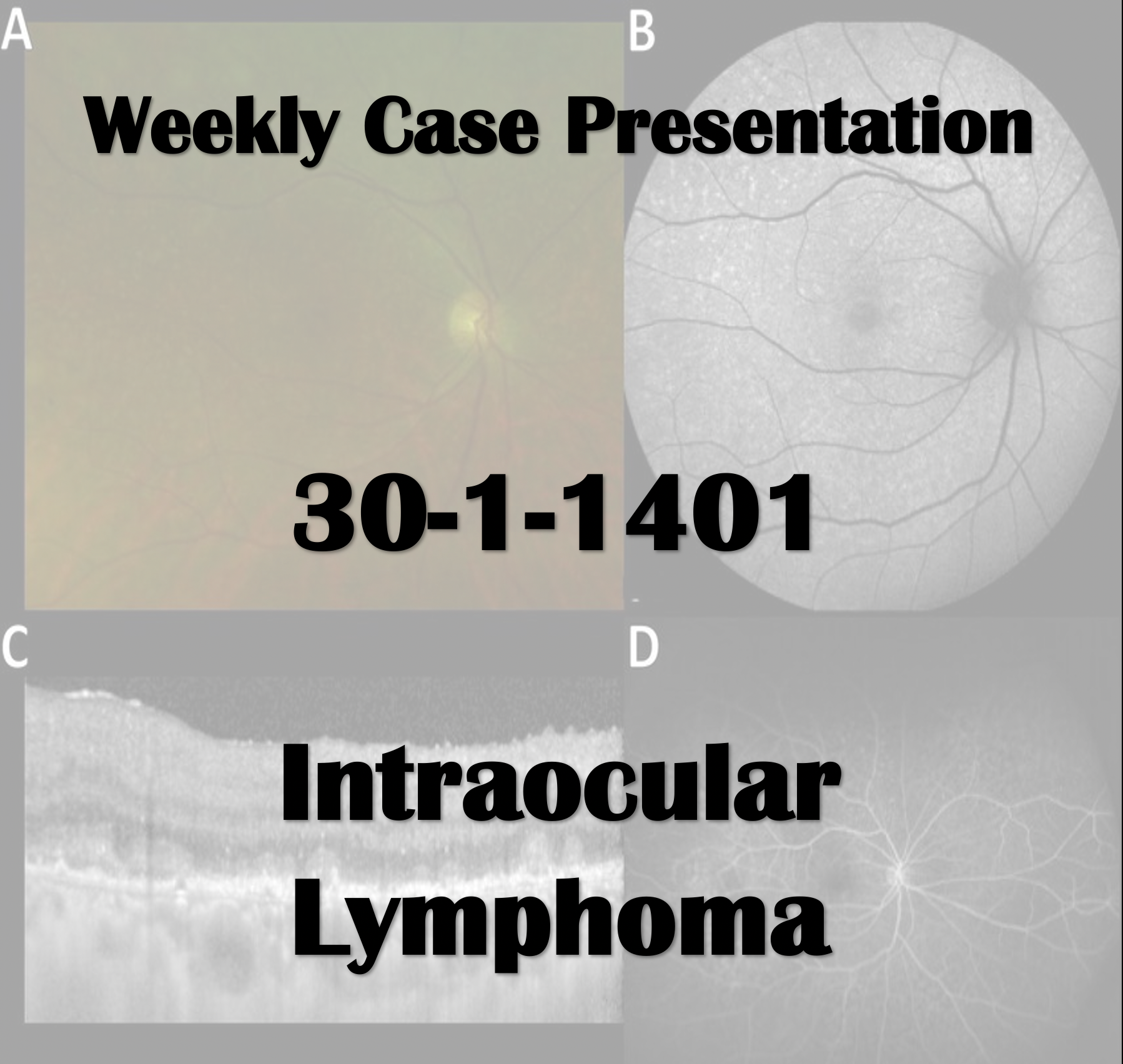
Posted inWeekly Case Presentation Weekly Case Presentation 30-1-1401 Weekly Case Presentation 30-1-1401 Special Thanks to Dr Riazi and Dr Banafsheh Afshan 2022-04-24
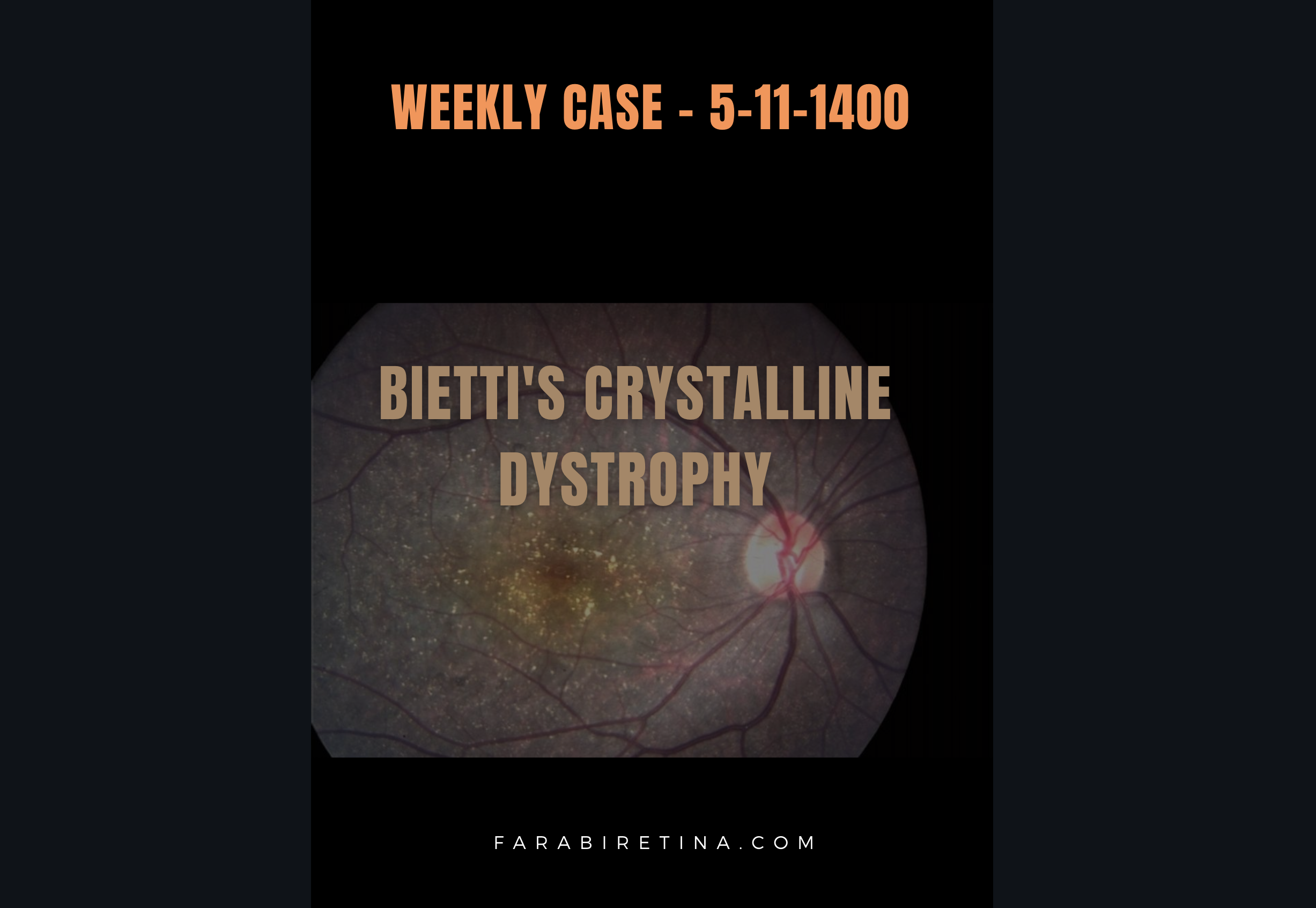
Posted inWeekly Case Presentation Weekly Case Presentation : 5-11-1400 Weekly Case Presentation : 5-11-1400 View Slides Here 2022-01-29
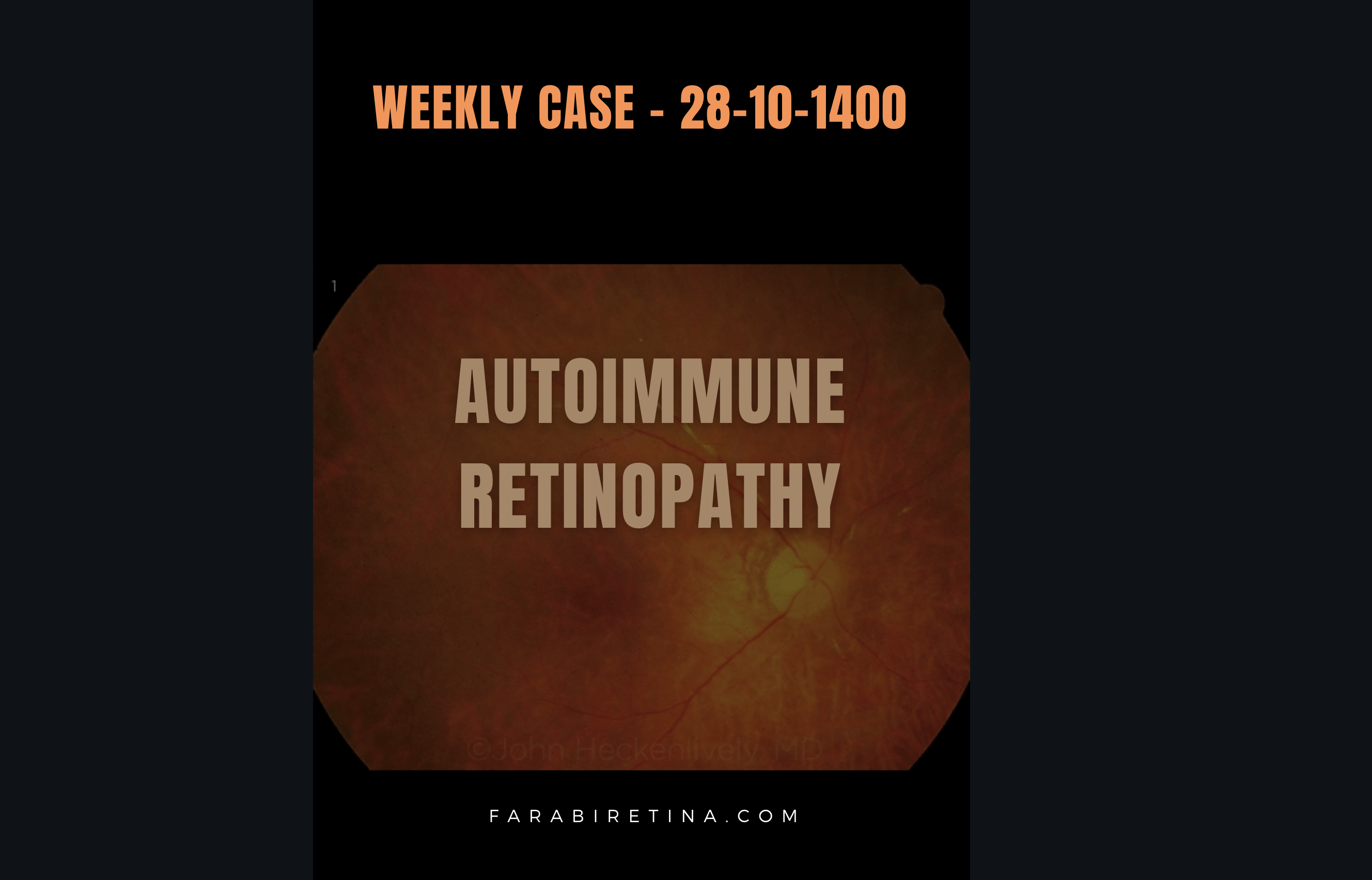
Posted inWeekly Case Presentation Weekly Case Presentation: 28-10-1400 Weekly Case Presentation: 28-10-1400 View Slides Here 2022-01-29
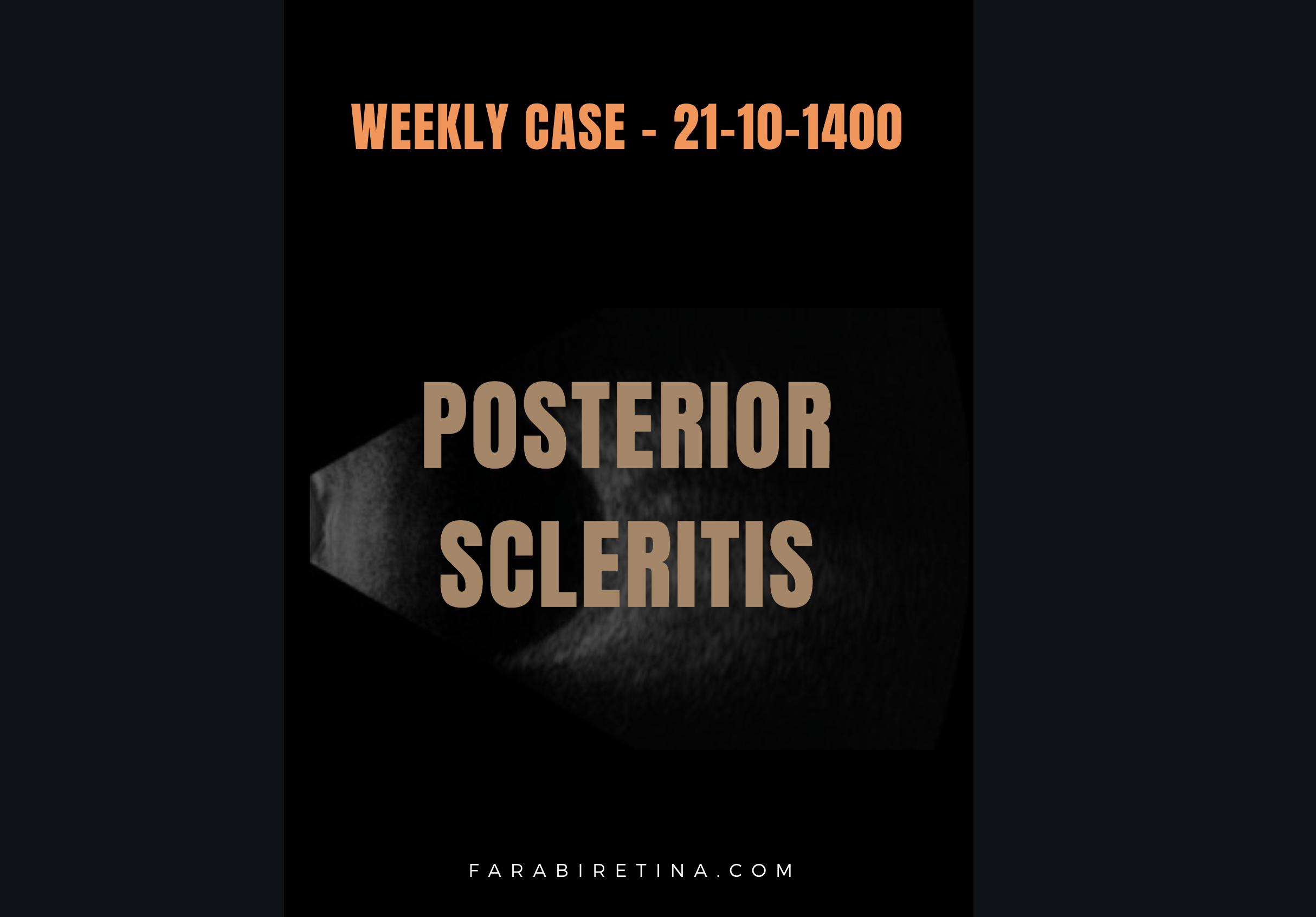
Posted inWeekly Case Presentation Weekly Case Presentation: 21-10-1400 Weekly Case Presentation: 21-10-1400 View Slides Here 2022-01-29
Posted inWeekly Case Presentation Weekly Case Presentation – 7-10-1400 Weekly Case Presentation - 7-10-1400 2022-01-16
Posted inWeekly Case Presentation Weekly Case Presentation 30-9-1400 Weekly Case Presentation 30-9-1400 2022-01-16
Posted inWeekly Case Presentation Weekly case Presentation – 16-11-2021 Weekly case Presentation - 16-11-2021 Atypical Presentations of Toxoplasmosis Special Thanks to Dr Asadi and Dr Khalili Pour 2021-11-16
Posted inWeekly Case Presentation Weekly Case Presentation 8-11-2021 Weekly Case Presentation 8-11-2021 Dr Banafsheh Afshan and Dr Riazi Ophthalmic Manifestations of COVID vaccination L View Slides below : 2021-11-13
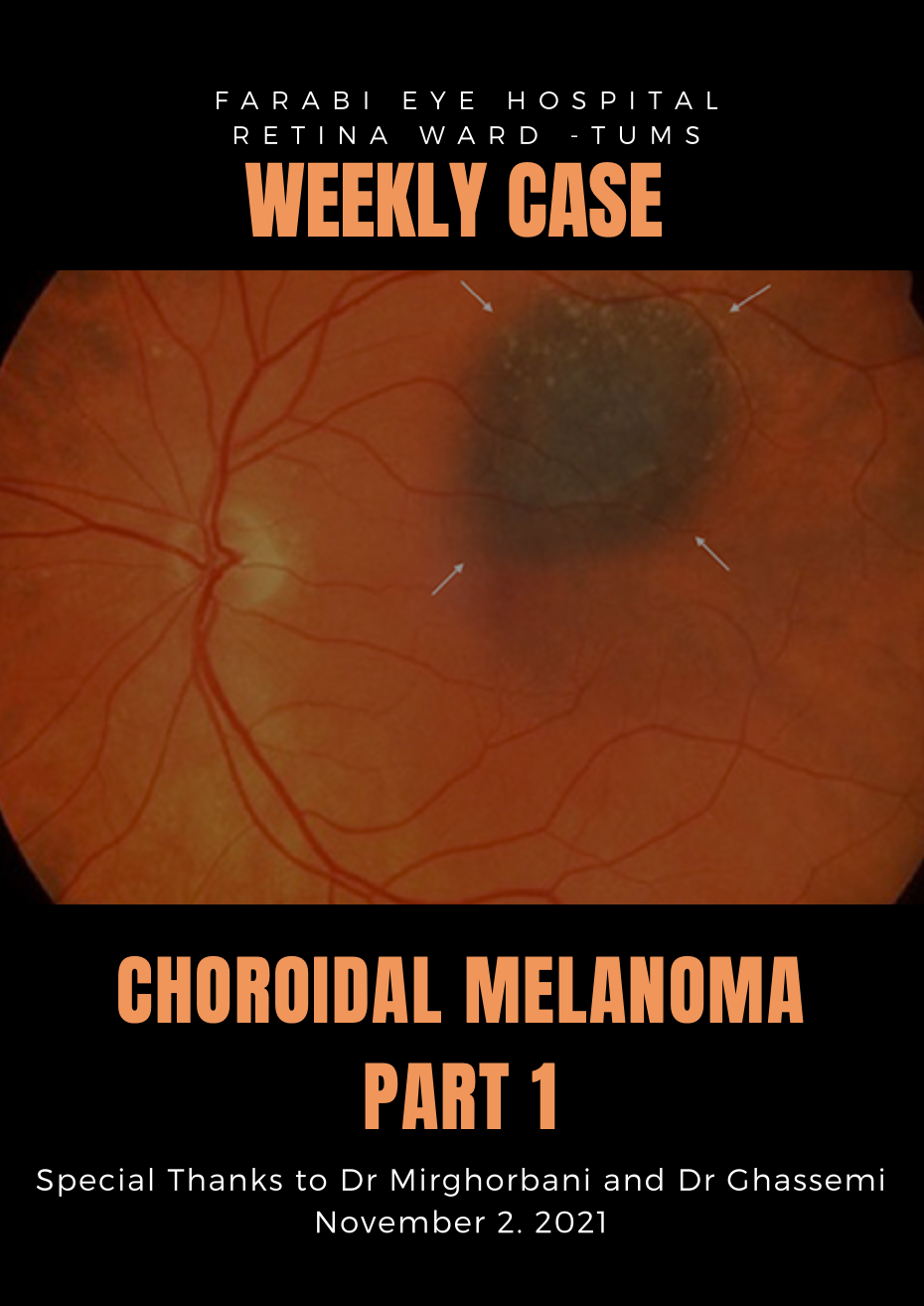
Posted inWeekly Case Presentation Weekly Case Presentation 2-11-2021 Weekly Case Presentation 2-11-2021 Updates on Choroidal Melanoma 2021-11-05
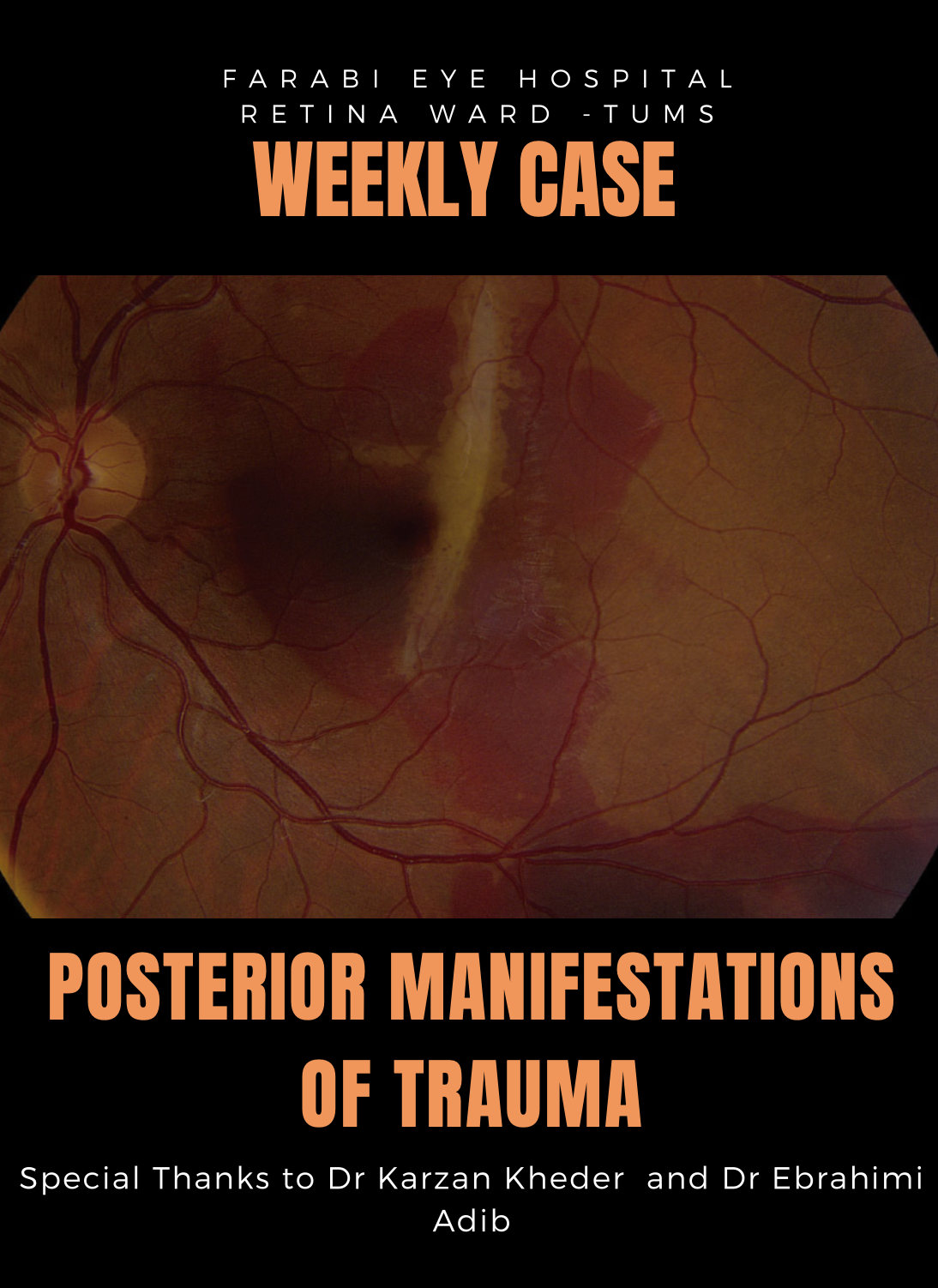
Posted inWeekly Case Presentation Weekly Case Presentation 26-10-2021 Posterior Manifestations of Trauma Weekly Case Presentation 26-10-2021 Special Thanks to Dr Kheder and Dr Ebrahimi Adib 2021-10-27
Posted inWeekly Case Presentation Weekly Case Presentation 12-10-2021 Weekly Case Presentation 12-10-2021 Different Manifestations of Retinal Arterial Macroaneurysm (RAM) 2021-10-13
Posted inWeekly Case Presentation Weekly Case Presentation 3-8-2021 Weekly Case Presentation 3-8-2021 Neuroretinitis Special Thanks to Dr Ebrahimi Adib and Dr Turkieh Reza 2021-08-05
Posted inWeekly Case Presentation Choroidal Lymphoma Weekly Case Presentation 20-7-2021 Special Thanks to Dr Mahdizad and Dr Riazi 2021-07-24
Posted inWeekly Case Presentation Weekly Case Presentation – 13-7-2021 Microcystic Macular Edema Special Thanks to Dr Mohammad Zarei and De Kheder 2021-07-13
Posted inWeekly Case Presentation Crystalline Retinopathy Weekly Case Presentaion 15-6-2021 Special Thanks to Dr Abbas Mohammadi and Dr Hamid Riazi 2021-06-15
Posted inWeekly Case Presentation Weekly Case Presentation Sickle Cell Retinopathy 6-8-2021 2021-06-08
Posted inWeekly Case Presentation Weekly Case Presentation 20-4-2021 برای مشاهده اسلایدها اینجا کلیک کنید 2021-04-22
Posted injournal club Weekly Case Presentation Choroidal Metastasis Weekly Case Presentation - 12-8-2020 Choroidal Metastasis -Special Thanks to Dr Ali Makateb and Dr Hamid Riazi https://www.aparat.com/v/RI53Z 2020-12-08